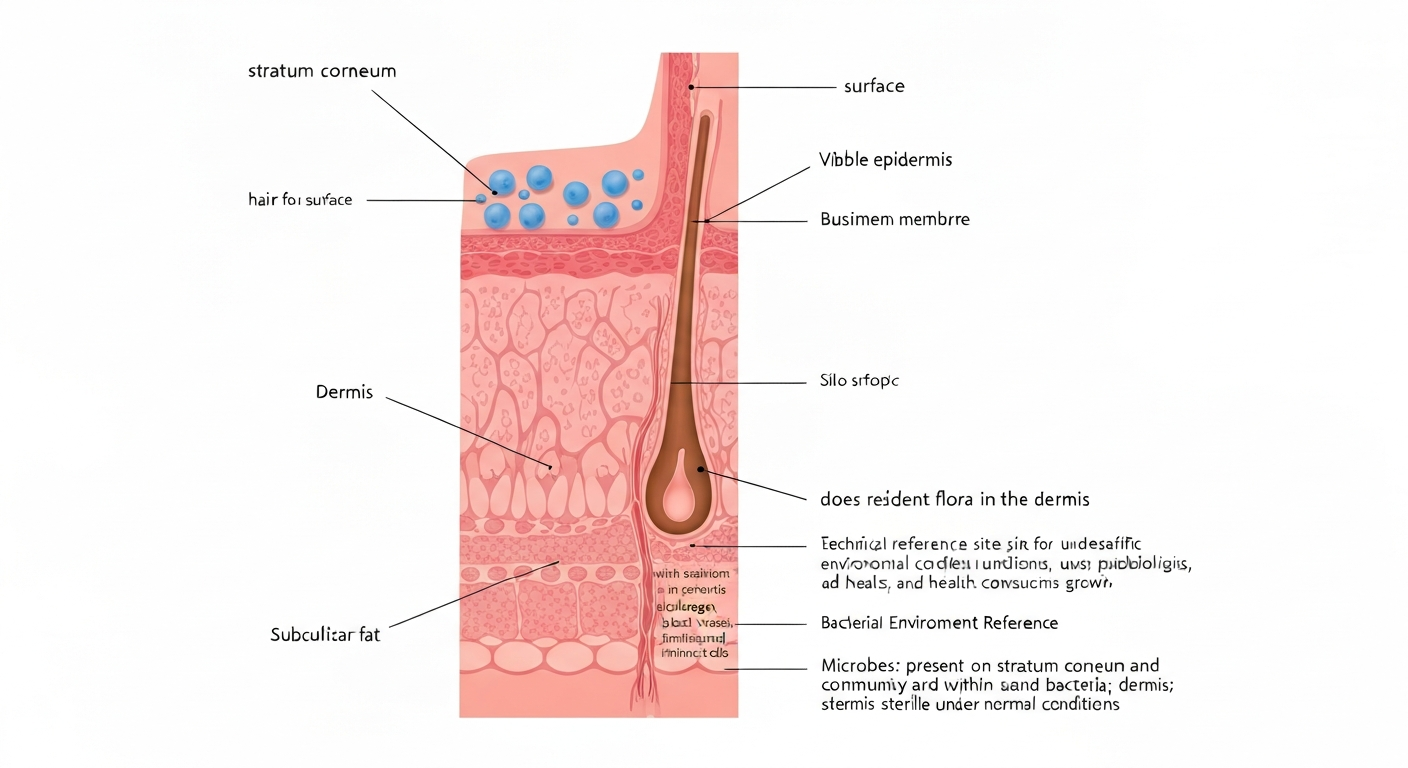
Resident skin flora does not normally grow in the dermis. In healthy skin, microbial colonization is restricted to the outermost dead layer of the skin (the stratum corneum) and the deeper portions of hair follicles and sebaceous glands. The living epidermis and the dermis below it are, under normal circumstances, sterile. When microorganisms do reach the dermis, it is because something has gone wrong: a physical breach, a compromised immune system, a medical device, or a highly invasive pathogen has overwhelmed the skin's layered defenses.
Does resident flora grow in the dermis: skin microbiome niches

Marcus Reeves
14 Jul 2026
The core question: dermis or epidermis?
People who study or work with skin microbiota often ask two related but distinct questions. First, does resident flora grow in the dermis? Second, does it grow inside the epidermis? The answers are different and depend on exactly which layer you mean. The epidermis has two functionally separate compartments: the stratum corneum (dead, keratinized cells at the surface) and the viable epidermis beneath it. Resident flora routinely occupies the stratum corneum. The viable epidermis is a different story, and the dermis more so. Understanding that distinction is the starting point for everything else in this article.
Resident versus transient flora: what the difference actually means
Resident flora (also called the resident microbiota or normal flora) refers to organisms that establish stable, long-term communities on a particular body site. They are consistently recoverable from the same location, they repopulate after removal, and they are adapted to local environmental conditions. On the skin, resident organisms include Staphylococcus epidermidis, Cutibacterium acnes, Corynebacterium species, and the yeast Malassezia. These are not just passing through; they have evolved strategies to survive the specific chemistry, temperature, and oxygen levels of skin surfaces and follicles.
Transient flora, by contrast, are organisms that land on the skin temporarily. They can survive for hours to days but do not establish stable communities under normal conditions. Transient flora matters enormously in infection control and food safety, because contamination events are almost always transient events. Knowing where transient flora grows and persists is a separate but related question worth exploring alongside this one.
The clinical relevance of this distinction is real. Resident organisms like S. epidermidis are generally low-risk in healthy hosts and can even suppress colonization by pathogens. But in a patient with a catheter, a surgical wound, or an immune deficiency, those same resident organisms can become opportunistic pathogens if they gain access to deeper tissue. The resident/transient distinction tells you about ecological niche; it does not tell you about virulence potential in every context.
Skin anatomy that controls where microbes can live
Skin is structured in a way that physically limits microbial access. Working from outside in, here is what microorganisms actually encounter.
Stratum corneum
The outermost 10 to 20 cell layers of the epidermis are composed of dead, flattened, protein-filled cells called corneocytes. This is the stratum corneum. It is the primary ecological zone for resident bacteria. The corneocytes are embedded in a lipid matrix and constantly shed (a process called desquamation), which physically removes microorganisms. The surface is dry by the standards of most bacterial growth media, acidic (pH roughly 4.5 to 5.5), and exposed to ultraviolet radiation on uncovered body sites.
Viable epidermis
Directly beneath the stratum corneum is the viable epidermis, made up of living keratinocytes. These cells are metabolically active and secrete antimicrobial peptides. Tight junctions between cells in the stratum granulosum layer act as a physical seal that prevents molecules (and microorganisms) from passing between cells. The basement membrane at the base of the epidermis is an additional structural boundary separating the epidermis from the dermis.
Pilosebaceous units and sweat glands
Hair follicles and their associated sebaceous glands are the most ecologically rich structures in the skin for microbial colonization. The follicular infundibulum (the opening of the follicle at the skin surface) connects the surface microenvironment to a deeper, lower-oxygen, lipid-rich environment inside the follicle. The deeper portions of follicles (the infrainfundibular region) are where Cutibacterium, in particular, thrives. Sweat gland ducts also open at the surface and have their own microenvironmental properties, including higher moisture and sodium chloride content.
Dermis
The dermis is the thick connective tissue layer below the epidermis. It contains collagen fibers, blood vessels, lymphatics, nerves, and a resident population of immune cells. In healthy skin, the dermis is sterile. Its vascularity means that any microorganism reaching the dermis is rapidly exposed to circulating immune components. The dermis is not a hospitable environment for resident flora under normal conditions; it is an immune-active tissue with resources to destroy pathogens quickly.
Where resident flora actually lives
Systematic skin microbiome studies, including the large-scale mapping work done as part of the Human Microbiome Project, consistently show that surface microbial communities are shaped by site physiology. The main niches for resident flora are the stratum corneum surface, the follicular infundibulum and deeper portions of hair follicles, and the sebaceous glands.
Within follicles, bacterial aggregates and biofilm-like structures have been visualized directly using fluorescence in situ hybridization (FISH) on plucked hairs and laser-capture microdissection of follicular compartments. These communities are not simply carried into the follicle from the surface; they have adapted to the follicular microenvironment and may not appear at all in a standard surface swab sample. This is one reason that the follicle is considered a reservoir, not just a conduit.
The sebaceous gland itself is particularly important. It produces sebum, and that lipid environment is chemically selective. Organisms that can tolerate or metabolize those lipids persist; others do not. Cutibacterium acnes is the textbook example of a follicle-specialized resident.
Why the living dermis stays sterile under normal conditions
Three overlapping defense systems maintain dermal sterility in healthy hosts, and they work together rather than as a single line.
- Physical and chemical barrier: The stratum corneum, corneocyte lipids, and the tight junctions of the viable epidermis physically block microbial transit. Antimicrobial peptides (including cathelicidin LL-37, beta-defensins, and RNase7) are secreted by keratinocytes and are active against a broad range of bacteria and fungi.
- Immune surveillance in the dermis: Dermal dendritic cells, macrophages, mast cells, and resident memory T cells are positioned throughout the dermis. Any microorganism that crosses the basement membrane encounters active immune detection and rapid response.
- Microenvironmental inhospitality: The dermis has different chemistry than the follicular or surface environment. It lacks the nutrient profiles (lipids, dead keratin) that resident flora depend on. Combined with immune pressure, there is simply no stable ecological niche there for organisms adapted to the skin surface.
The result is that in a healthy individual with intact skin, the dermis remains sterile not because microorganisms never arrive at its borders, but because the defenses at every layer prevent them from establishing.
The physical and chemical conditions that shape skin's resident community
Skin is not a uniform surface. Sebaceous sites (face, upper chest, back) are chemically very different from moist sites (axillae, groin, toe webs) or dry sites (forearms, palms). These differences drive community composition as reliably as temperature and pH drive community composition in food environments.
| Condition | Typical Value or Range | Effect on Microbial Community |
|---|---|---|
| Surface pH | 4.5–5.5 (acidic) | Selects for acid-tolerant residents; suppresses many transient pathogens |
| Surface temperature | ~32–34°C | Below core body temperature; favors organisms adapted to skin-range temps |
| Follicle/sebaceous O2 | ~0.1–2.5% O2 | Microaerophilic/anaerobic niche; strongly favors Cutibacterium |
| Sebum lipid composition | Triglycerides (~30–50%), wax esters (~20–30%), squalene (~10–20%), free fatty acids | Nutrient and selective pressure; favors lipid-metabolizing taxa |
| Surface moisture (TEWL/hydration) | Variable by site; moist folds > dry forearms | Higher moisture at folds supports Gram-negative and fungal taxa |
The low oxygen tension inside follicles deserves emphasis. Measurements and reviews place follicular and sebaceous pO2 in the range of roughly 0. Physiological skin oxygen levels: An important criterion for skin cell functionality and therapeutic approaches (review summarizing tissue pO2 including follicles/sebaceous glands) reports follicle and sebaceous gland pO2 values of roughly 0.1–2.5% O2, consistent with a microaerophilic to anaerobic niche. 1 to 2.5% oxygen. That is close to anaerobic by practical microbiology standards. Organisms that need atmospheric oxygen cannot sustain communities in that niche, which is why the obligate anaerobe Cutibacterium dominates sebaceous follicles while aerobic Staphylococcus species dominate the skin surface.
The common resident taxa and where each one actually lives
The Human Microbiome Project and follow-up topographic studies identified the same core taxa repeatedly across multiple body sites. But 'found on skin' covers very different ecological positions depending on the organism.
Cutibacterium (formerly Propionibacterium)
Cutibacterium acnes is the dominant organism in sebaceous follicles. It is a Gram-positive, anaerobic to microaerophilic rod that metabolizes triglycerides in sebum, releasing free fatty acids. Its preferred niche is the deeper portions of the pilosebaceous unit, specifically the infrainfundibular region, where oxygen is lowest and sebum is most concentrated. Surface swabs often underestimate C. acnes; follicular sampling methods recover it at much higher proportions.
Staphylococcus epidermidis and other coagulase-negative staphylococci
S. epidermidis is the most consistently detected organism across virtually all skin sites. It colonizes the stratum corneum surface and the upper portions of follicular infundibula. It is a facultative anaerobe, tolerates the acidic surface pH, and can form biofilms. It is not specialized for the deep follicular niche the way Cutibacterium is, but it is a generalist that tolerates a wide range of skin surface conditions.
Corynebacterium
Corynebacterium species dominate moist skin sites (axillae, toe webs). They are Gram-positive, aerobic to facultatively anaerobic rods that hydrolyze apocrine and eccrine sweat components. Their preference for moist environments mirrors how moisture affects community composition in food environments: water activity drives selection.
Malassezia
Malassezia is a lipid-dependent yeast (it requires exogenous fatty acids for growth) and is therefore concentrated at sebaceous sites: the scalp, face, and upper trunk. It occupies the surface stratum corneum and upper follicle. Unlike bacterial residents, it is a fungus, but it follows the same environmental logic: lipid availability selects for organisms that can use lipids. For information on growth sites of another clinically important yeast, see where does Candida auris grow.
Other residents
Dry sites host sparser communities dominated by beta-Proteobacteria and some Firmicutes. Gram-negative organisms including Acinetobacter are recoverable from forearms and other dry sites. The overall picture is one of environmental filtering: each site's temperature, pH, moisture, lipid content, and oxygen level determine which organisms persist.
Can resident flora grow inside the epidermis, and when does it?
This is where the question gets more nuanced, and where recent molecular data have added complexity without overturning the basic model.
Stratum corneum colonization is normal and expected
The stratum corneum is, strictly speaking, part of the epidermis. So in the narrow sense, resident flora does live inside the epidermis: it lives in the outermost dead layers of it. Nobody disputes this. The question becomes interesting when you ask whether organisms cross into the viable epidermis below, or deeper still into the dermis.
Follicular reservoirs extend into the dermis anatomically
Hair follicles extend from the skin surface down through the entire epidermis and into the dermis. Bacteria that colonize the deep portions of follicles are, anatomically, sitting in a structure that passes through the dermis. However, they remain within the follicular lumen, surrounded by the follicular epithelium. This is not the same as colonizing the dermal connective tissue itself. The follicle is best understood as an infolding of the epidermis: a tube that physically passes through the dermis but that maintains its own epithelial lining and its own immunological interface with the surrounding tissue.
Molecular signals below the basement membrane: what the evidence shows
A notable 2013 study by Nakatsuji and colleagues used laser-capture microdissection (LCM), quantitative PCR, fluorescence in situ hybridization, and 16S sequencing to detect bacterial signals in dermis and subcutaneous adipose tissue from normal facial skin. They reported low but reproducible 16S DNA signals below the basement membrane, including in dermis and subcutaneous adipose. The study was methodologically careful: it included non-tissue controls, muscle tissue controls, and multiple detection modalities.
This finding has not been comprehensively replicated, and it sits in tension with the immunological and barrier data that support normal dermal sterility. It also sits against a broader methodological concern in the field: low-biomass tissue samples are extremely vulnerable to contamination from reagents, the sectioning environment, and DNA carry-over. The phenomenon of 'kitome' contamination (where commercial DNA extraction kits introduce spurious microbial DNA) and 'splashome' contamination (from the sectioning environment) are documented problems that can produce false-positive signals in exactly this type of experiment. Tools like decontam are now commonly used to identify likely contaminant sequences in low-biomass datasets, but they require well-designed negative controls to work properly.
A viability-resolved study from 2023 using propidium monoazide digital droplet PCR (PMA-ddPCR) and FISH found that viable bacteria are concentrated in follicles, while much of the 16S signal on the skin surface represents extracellular or non-viable DNA. This is an important methodological insight: detecting DNA is not the same as detecting live organisms. It is plausible that some of the 'dermal' signals detected in PCR-based studies represent extracellular microbial DNA that has migrated from the follicular compartment or the surface, not viable colonizing organisms. PMA-based methods themselves have documented limitations in low-biomass or community-complex samples, so the picture is not fully resolved.
The working conclusion from the available evidence is that the dermis does not host a stable, viable resident microbial community in healthy skin. Molecular signals below the basement membrane are real in some studies but their biological meaning remains uncertain, and the technical challenges of low-biomass tissue microbiome work mean caution is warranted before interpreting them as evidence of true dermal colonization.
When microorganisms do enter the dermis
Dermal invasion by microorganisms happens under specific, identifiable conditions. See where does anthrax grow for an example of a pathogen (Bacillus anthracis) that thrives as spores in soil and can cause cutaneous infection if spores enter skin breaches. Understanding these is more clinically useful than debating whether trace DNA signals represent colonization.
- Physical trauma: cuts, abrasions, punctures, and surgical wounds create direct pathways through the epidermal barrier into the dermis. Resident flora (especially S. epidermidis and C. acnes) can become opportunistic pathogens via these routes.
- Medical devices: indwelling catheters, implants, and sutures provide a continuous surface that microorganisms can track from the skin surface into subcutaneous and deeper tissue. Biofilm formation on device surfaces is a major mechanism.
- Immunosuppression: patients with reduced innate or adaptive immunity cannot maintain normal dermal surveillance. Organisms that would be cleared instantly in a healthy host can establish themselves in deeper tissue.
- Highly invasive pathogens: organisms like Staphylococcus aureus, Streptococcus pyogenes, and others (including anthrax-causing Bacillus anthracis, a separate organism worth understanding in its own context) carry specific virulence factors that actively overcome barrier defenses.
- Folliculitis and follicular rupture: when a follicle is damaged or ruptures (as in acne vulgaris), follicular contents including viable C. acnes are released directly into the surrounding dermis, triggering the inflammatory cascade seen in inflammatory acne lesions.
Detection and sampling: why method matters for answering this question
What you find in a skin microbiome study is largely determined by how you sample. Surface swabs and tape strips recover stratum corneum organisms predominantly and provide little information about follicular communities. Plucked hairs and follicular expression methods recover follicle-associated organisms, including deep Cutibacterium populations, that swabs miss entirely. Sterile punch biopsy followed by LCM allows targeted sampling of specific tissue layers but introduces serious contamination risk that requires rigorous controls (sampling blanks, extraction blanks, no-template PCR controls, and statistical contaminant filtering).
Culture-based methods have their own biases: many skin residents (including slow-growing anaerobes and fastidious lipid-dependent organisms) are difficult to cultivate on standard media. Molecular methods like 16S amplicon sequencing and metagenomics detect broader community diversity but do not distinguish viable from non-viable organisms without additional steps like PMA treatment. Each method answers a different question, and comparing studies that used different approaches requires understanding those differences.
Practical implications for infection prevention and decolonization
For clinicians and infection preventionists, the key takeaway is that resident flora does not need to be in the dermis to cause dermal infection: it just needs a route in. The most effective prevention strategies target that route rather than attempting to eliminate the resident community, which is ecologically stable and, in most cases, protective.
Antiseptic skin preparation before surgery or device insertion is effective precisely because it temporarily reduces surface and follicular organism counts, reducing the inoculum available to contaminate a wound or device track. Chlorhexidine-based preparations have demonstrated efficacy in reducing S. epidermidis and other residents at surgical sites, though follicular populations are harder to reach and can repopulate quickly. Understanding that follicles are a reservoir, not just a surface, matters for choosing contact time and concentration.
For food safety professionals and microbiologists thinking about skin as a contamination source, the same ecological logic applies: transient organisms on the surface are the primary contamination risk during food handling, while resident organisms are a secondary but real concern during breaches (cuts, abrasions) that might transfer deeper-seated organisms. Related reading on fungal food contaminants explains how mycotoxins can grow on a variety of foodstuffs and why that matters for food safety. Good hand hygiene and barrier protocols address the transient flora risk; understanding resident flora ecology helps assess what is realistically present and how to interpret contamination events.
Decolonization of specific resident organisms (for example, nasal S. aureus decolonization with mupirocin before orthopedic surgery) works because it targets a specific organism in a specific niche using a targeted antimicrobial, not because it disrupts the entire skin ecosystem. Broad-spectrum decolonization of the skin resident flora is neither practical nor desirable: resident organisms occupy a niche that pathogenic organisms would otherwise fill.
FAQ
Does resident skin flora normally grow in the dermis?
In healthy, intact human skin the living dermis (and the viable epidermis beneath the stratum corneum) is generally sterile of growing microbial populations. Standard dermatology and microbiome reviews and large-scale mapping (Human Microbiome Project, Grice/Segre) show that resident microbes are concentrated on the stratum corneum and in skin appendages (hair follicles, sebaceous and eccrine glands). Low-level 16S signals reported from dermal biopsies in some studies should be interpreted cautiously because of low biomass and contamination risks; when viable organisms are demonstrated, they are most often located in follicular or appendageal compartments rather than the interstitial dermis (see Nakatsuji et al. 2013 and later viability-resolved work).
Where on and in the skin do resident microbes normally colonize?
Resident (commensal) skin flora typically colonize: - The stratum corneum and adherent corneocytes on the skin surface. - Pilosebaceous units (hair follicles and sebaceous glands) and follicular canal contents. - Sebaceous and moist glandular niches (sebaceous-rich sites favor Cutibacterium; moist sites favor Staphylococcus and Corynebacterium). These niches provide nutrients (lipids), lower oxygen, and protected microenvironments that support viable bacterial communities and sometimes biofilms.
How are resident and transient flora defined and how do they differ?
Resident flora (commensals) are microbial taxa that persist for long periods at particular skin sites, are adapted to local conditions, and reproduce there (e.g., Cutibacterium in follicles, Staphylococcus epidermidis on skin). Transient flora are microbes that appear temporarily from environmental contact, fomites or other people; they may survive on the surface for hours to days but do not establish a stable population. The operational difference matters clinically: resident organisms are normal members of the skin ecosystem and often low risk in intact skin, whereas transient organisms can be indicators of contamination and (if pathogenic) potential sources of infection given a breach.
Why is the viable dermis normally sterile?
Multiple interacting barriers keep the viable dermis microbe-free in healthy individuals: - Physical barrier: intact stratum corneum, tight junctions in the epidermis and corneocyte lipid matrix limit penetration. - Chemical barrier: acidic surface pH, antimicrobial peptides (LL-37, defensins, RNase7) and antimicrobial lipids produced by keratinocytes and glands. - Immune surveillance: dermal immune cells (dendritic cells, macrophages, resident T cells) and a vascular supply rapidly clear microbes that breach the epidermis. These defenses plus lack of suitable nutrients/oxygen in interstitial dermis normally prevent colonization and growth.
What physical and chemical conditions on skin select for particular taxa?
Key environmental parameters and their effects: - pH: skin is acidic (~4.0–5.5), selecting for acid-tolerant taxa. - Temperature: surface & follicle temperatures ~32–34°C support human-associated bacteria. - Moisture: moist sites (intertriginous areas) favor Corynebacterium and Staphylococcus; dry sites have lower biomass and greater diversity. - Lipids: sebum-rich follicles provide triglycerides, wax esters and free fatty acids that favor lipophilic and lipid-metabolizing taxa such as Cutibacterium. - Oxygen: follicular and sebaceous microenvironments are microaerophilic to anaerobic (low pO2), selecting for facultative anaerobes and anaerobes (Cutibacterium). These parameters explain site-specific communities reported in skin microbiome surveys.
Are there reliable methods to tell if bacteria detected below the epidermis are viable residents or contamination/artifact?
Distinguishing viable, resident microbes from DNA fragments or contaminants requires method choice and controls: - Viability-resolving methods: culture, fluorescence in situ hybridization (FISH), and PMA-treated sequencing (PMA-ddPCR/PMA-seq) can indicate intact cells, but PMA methods have technical limitations and require optimization. - Visual methods: FISH or immunostaining on plucked hairs, follicles or LCM sections can localize cells. - Culture from sterilely obtained biopsy or follicle contents demonstrates live organisms but can miss fastidious taxa. - Critical controls: sampling blanks, extraction blanks, no-template PCRs, randomized processing and bioinformatic contaminant removal (e.g., decontam) are essential for low-biomass tissue work to rule out kit/reagent contamination. Combining multiple orthogonal approaches (visualization + viability assays + culture + strict controls) gives the most reliable evidence of genuine subepidermal residency.
Next Article
Can Bacteria Grow in Lemon Juice? Growth Risk Explained
Learn if bacteria can grow in lemon juice, how acidity affects survival vs multiplication, and safe storage steps.
